HEART RHYTHM CLINIC
Looking after your heartHOME | ABOUT US | THE TEAM | TREATMENTS & PROCEDURES | COST | APPOINTMENTS | CONTACT US
Catheter Ablation
Catheter ablation Procedure
Catheter ablation is performed in people who have been diagnosed with an abnormal heart rhythm that has not responded to medication.
Your heart rhythm abnormality is likely to be due to an area of extra electrical activity or short circuit. In your heart, electrical impulses bypass the normal conduction pathway through the heart and use an extra electrical pathway or arise from a group of cells (foci) instead. This procedure aims to stop such abnormal mechanisms and provide relief from the symptoms you have been experiencing.
The procedure
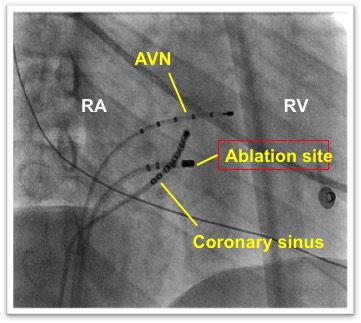
Catheter ablation is a clinical technique whereby the doctor applies radiofrequency (heating) energy or cryothermal (freezing) energy directly onto the area responsible for the extra electrical focus or circuit within your heart.
The use of ablation energy causes scar tissue to form, which blocks the area from generating or conducting the fast impulses that cause your arrhythmia. Therefore, the normal conduction pathway takes over and your heart rhythm returns to normal.
This procedure is usually performed under a local anaesthetic, with sedation, which will help you to relax. Paediatric ablation is performed under general anaesthesia. X-ray screening is used during the procedure so if you think you may be pregnant you should let us know before the procedure.
Success of ablation
The catheter ablation procedure is successful in the great majority of cases. The success rate depends on where the problem is within your heart. Your doctor will discuss the success rate of your particular procedure with you on an individual basis before you sign your consent form. If the procedure is unsuccessful it may be possible to repeat it at a later date.
Risks of the procedure
Catheter ablation is safe; however as with any procedure there are potential risks. The risks will be fully explained by our doctors before you have your procedure. Radiofrequency ablation is performed safely in both children and adults.
All the risks outlined below can be treated and are rarely life threatening.
- Bruising and bleeding: this is common in the groin following the procedure. This usually disappears within a week and does not cause a problem.
- Blood vessel damage: occasionally the catheter electrodes can accidentally damage the blood vessels when being moved into position within the heart. The risk of this happening to you is between 3% and 5%. Serious injury to the blood vessels requiring a surgical procedure to repair the damage is extremely rare and occurs in less than 1% of patients.
- Pneumothorax: very occasionally the catheter electrodes can puncture the lung wall. Air leaks out of the lungs and collects in the space between the lung and chest wall, resulting in partial or complete collapse of the lung. If this happens the doctor may need to insert a drain to re-inflate your lungs. The risk of this happening to you is less than 1%
- Haemothorax: very occasionally the catheter electrodes can puncture the lung wall. Blood leaks out of the lungs into the pleural cavity, the space between the lungs and the walls of the chest. If this happens the doctor will need to insert a drain to re-inflate your lungs. The risk of this happening to you is less than 1%
- Pulmonary embolism or stroke: the risk of developing blood clots that travel to the lungs (pulmonary embolism) or brain (stroke) is extremely rare, less than 1%.
- Palpitations: it is common to experience palpitations (extra heart beats) during the procedure, due to the catheter electrodes stimulating your heart. Your heartbeat will usually return to its normal rhythm very quickly without needing further treatment. However, very occasionally extra treatment (cardioversion) is needed to correct your arrhythmia. Cardioversion is a treatment for heart rhythms that are irregular. You will be given a short-acting sedative to make you sleepy. Once you are asleep a defibrillator is used to send electrical energy to the heart muscle to restore the normal rhythm and rate.
- Cardiac tamponade: during placement, the catheters may puncture the heart muscle causing blood to collect around the heart. If this happens the doctor may need to insert a drain to remove it. The risk of this happening to you is less than 1%; this risk increases slightly if your doctor needs to make a transeptal puncture.
- Transseptal puncture: during the procedure it is sometimes necessary for your doctor to make a small hole in the middle membrane (transseptal puncture) between the top heart chambers in order to gain access to the left side of the heart. This hole will usually seal up quickly after the procedure.
- Heart block: very occasionally the radiofrequency ablation catheter can damage your heart’s own conduction system. If the hearts normal conduction pathway is partly or completely blocked, a rhythm called heart block may develop which results in failure of the electrical impulses to travel through the AV node from the atria to the ventricles. If this happens you will need a permanent pacemaker fitted before you leave hospital to maintain a normal, regular heartbeat. The risk of needing a permanent pacemaker is less than 1%. However, if you have an extra pathway located close to the AV node there is an increased risk of between 1 and 2%.
- Palpitations post procedure: you may also experience them on and off for a few weeks after the procedure, until the small scars created in the heart heal. Sometimes, you may feel as if your abnormal heart rhythm is returning, but then it suddenly stops. These sensations are normal and you should not be alarmed. However, if you feel your abnormal heart rhythm has returned, you should call your GP.
Before admission
If you are taking medication to control your heart rhythm the admission co-ordinator may advise you to stop taking your tablets five days before your procedure. This is to allow your doctor to make a better assessment of your heart rhythm. Stopping your tablets may cause your symptoms to return.
If you are taking warfarin (blood thinner) regular blood tests will be needed for at least four weeks before the procedure, usually at your doctor’s surgery. We ask that you keep your INR between 2.0 and 3.0. A record of this should be kept in your yellow warfarin book. We also request that you check your INR three days before your admission to confirm it is in this range to enable the procedure to go ahead.
If you are taking alternatives to warfarin, such as apixaban, dabigatran, edoxaban or rivaroxaban, your consultant will advise you with specific instructions about continuing these medications leading up to the procedure.
If you have any questions please talk to our secretary about the medicines that you are currently taking.
Before the procedure
On your arrival to the ward a nurse will talk to you and your family about your hospital admission and answer any questions you may have. Before the procedure, you will have blood tests taken and an electrocardiogram (ECG) recorded. A doctor will also see you to explain the procedure to you, and ask you to sign a consent form to ensure you understand the procedure and the associated risks. If you have any worries or questions please do not be afraid to ask. It is important to tell your nurse or doctor if you have any allergies or have had a previous reaction to drugs or other tests. If you are having the procedure done under a general anaesthetic, you will also talk to an anaesthetist.
A doctor or nurse will need to insert a small needle into a vein in your hand (cannula) in order to give you drugs during the procedure. You will also be asked to shave your groin and if necessary your upper chest and you will then be given a hospital gown to wear.
You will not be allowed to eat or drink anything for four hours before your procedure. If you are diabetic, your nurse will discuss your tablets/insulin dose with you, because not eating may affect your blood sugar levels.
The procedure could take a couple of hours. You may wish to let your family know so that they do not worry.
During the procedure
You will be taken to the catheter lab where a nurse will stay with you and be there to reassure you throughout the procedure. There is a lot of equipment in the room, which is used to monitor your heart rhythm. You will be awake during the procedure, but to help you relax your doctor will give you a short acting sedative.
The doctor will inject a local anaesthetic into your groin to numb your leg. This may sting a little and you may feel some mild discomfort. When the local anaesthetic has taken effect, the doctor will insert a small tube (sheath) into your groin. You should not feel any pain, but let your doctor know if you do. Through the sheath the doctor will gently thread several flexible wires (catheter electrodes) into your heart. These special wires will record and ablate (destroy) the extra electrical signals from within your heart. The type of arrhythmia you have, will determine how many wires your doctor will use for your ablation. The catheters are about the size of a small drinking straw. The doctor carefully moves the catheters into different positions within your heart under x-ray screening (sometimes, your doctor may also put a catheter into one of your veins below your shoulder blade). You should not feel pain during this part of the procedure.
Once the catheters are in place, your doctor will attempt to start your arrhythmia by giving your heart small electrical impulses (paced beats) to make it beat at different speeds. This allows the doctor to collect detailed information about the cause of your arrhythmia and pinpoint where the area of extra electrical activity responsible for your arrhythmia is within your heart. During this time you may feel your heart speeding up, slowing down or missing a beat. This may cause you some mild discomfort. However, this is a normal part of the procedure and in the controlled setting of a radiofrequency ablation is not a danger to you. Sometimes, your doctor may also need to give you drugs to bring on your arrhythmia. The doctor will use the ablation catheter to deliver a small amount of heating or freezing energy directly onto the area of extra electrical activity to create a scar.
You may feel a slight burning sensation or heaviness in your chest during this part of the procedure.
The formation of scar tissue as a result of radiofrequency ablation will not interfere with the normal conduction or function of the heart. This means that after ablation your heartbeat will only follow the normal electrical pathway.
If you experience any symptoms during the procedure, for example, chest pain, dizziness, shortness of breath, please tell your nurse or doctor.
After the doctor has performed the ablation, you will be kept in the catheter lab and continue to be monitored for approximately 20 minutes. The doctor will then stimulate your heart again in an attempt to start your arrhythmia. If this is not possible the ablation is considered a success.
After the procedure is completed the catheter and IV line will be removed. Firm pressure will be applied to your groin where the catheter was inserted to stop you from bleeding.
After the procedure
After the procedure you will be moved to the recovery area where you will be monitored for a short time. On returning to the ward you will need to rest for a few hours. You may feel a little sleepy until your sedative has worn off. The nurse will record an ECG, check your blood pressure, pulse and feel your foot pulses. The nurse will also check your groin for any bleeding. It is important that you remain in bed and avoid bending your affected leg for approximately two hours after the catheters have been removed. This is to prevent any bleeding from the puncture site. After this time you will be able to get up if there are no complications.. You will be able to eat and drink normally as soon as you return to the ward. The nurse will remove the small needle in your hand. If you feel any palpitations or dizziness after the test, please let the nurse know. You may also have a chest x-ray to make sure that you do not have a pneumothorax (pocket of air) in your lung.
Results
Your doctor will usually discuss the results and ongoing treatment plan with you and your family after the procedure.
Going home
You will normally be able to go home on the same day or the following day. It is important to ask a family member or friend to collect you and drive you home. If you are being discharged home the same day as your procedure we would advise you to have someone stay with you for the night. Before going home, your consultant will advise you regarding the medicines you will need to take, or stop and your follow-up care.
Caring for your wound
You will have a small dressing on your puncture site that can be removed the next day. It is important to keep the area clean and dry until it has healed. If you notice any swelling, redness or oozing please let your GP know.
Resuming normal activities
You can resume your normal daily activities when you leave hospital. You should not strain or lift heavy objects for a few days so the incision site can heal. Unless your job requires you to lift heavy objects, you can return to work in a day or two. You should not drive a car for one week. If you hold a Group 2 PSV licence (lorries/buses) you are not allowed to drive for six weeks.
Follow-up care
Our cardiac rhythm management team will give you specific follow-up instructions when you leave hospital. Our doctors will write a detailed letter to your GP describing your hospital stay and treatment.
Further information
The following websites also provide useful information:
TREATMENTS & PROCEDURES:
THE TEAM
Our specialist doctors are here to guide you through every part of your procedure
TREATMENTS & PROCEDURES
Learn more about the treatment or procedure you are about to have
FREQUENTLY ASKED QUESTIONS
Without a doubt you will have questions, check out this handy resource
CONTACT US
Heart Rhythm Clinic is based at Spire Southampton Hospital but also consults in Lymington, Sarum Road (Winchester) and the Nuffield Hospital, Southampton.